Why the WHO report on congenital anomalies in Iraq is a disgrace

The recently published World Health Organization report on its study of congenital birth anomalies in Iraq is nothing short of a disgrace.
There have been an increasing number of reports about childhood
cancers, adult cancers and birth defects in Iraq. Public
pressure and media attention to this catastrophic situation
prompted a joint study by the World Health Organization (WHO) and
the Iraqi Health Ministry to determine the prevalence of birth
defects in the country. The study began in May-June 2012 and was
completed in early October 2012. But it was not made public until
recently. And I have to say that those who designed and carried
out the study were well aware that the method they chose could
not possible give correct answers to the question of congenital
anomaly rates, since they had consulted with me before they
started, and I had pointed out why their method was unsafe, even sending
them a report suggesting a method that would work.
In May 2011, I was asked to travel to Geneva by the Union of Arab Jurists to make my first presentation at the UN Human Rights Council, reporting our preliminary findings of extraordinarily high rates of cancer, infant mortality and sex ratio perturbations in the population of Fallujah, which we published in the International Journal of Environment and Public Health in 2010. I met with the director of the Human Rights Council, and also with the director of the International Red Cross, and made the case for intervention.
There was massive anecdotal evidence of these genetic damage effects of the US uranium weapons since the mid-1990s and in Fallujah after the 2004 war, but no one had carried out any study. We collected some money from individuals (about £4,000) and marched in. What we found made headlines in The Daily Telegraph, Le Monde and all over the world. In that study, we examined infant mortality rather than congenital birth defects, for reasons we gave in the paper and I will review here.
Later we also published two other follow-up studies based on hospital data, one analyzing 52 elements in the hair of the parents of children with congenital anomalies, the other giving the congenital anomaly rates and types. Both were based on prospective collection of data by the pediatricians from Fallujah General Hospital, and so we could be sure of the types of anomaly and the numbers.

I have to say that the fear generated by these discoveries made it extremely difficult to get the results published. The Lancet threw the papers out without sending them for review. The International Journal of Environment and Public Health was attacked after the first one, by various individuals they refused to name – and they wouldn’t publish the second one, which was published by Conflict and Health. The third one was also rejected by The Lancet and various other frightened journals and eventually was published by the Journal of the Islamic Medical Association, and then only after I asked them what Allah would think of their pusillanimous behavior. So much for scientific truth.
I pointed out to the WHO representative who contacted me in January 2011, Syed Jaffar Hussein, asking if I would join the WHO project, that the kind of questionnaire study that WHO were proposing would fail for two reasons. The first and most critical is that parents will not have sufficient knowledge to diagnose a congenital anomaly in their baby. For example, in the absence of hospital involvement at a high technical level (e.g. Fallujah Hospital) the baby will just die of what seems to the parents to be pneumonia, or failure to thrive, or the child will die for no apparent reason. In terms of congenital heart defects, or kidney defects, or many neurological defects there is no observable sign. And the type of monstrous defect, the Cyclops eye, the lack of arms, all the pictures on the Internet, these are a minor fraction of all the congenital defects that are fatal at birth. Generally the mother is not allowed to see such a baby and she is told it has died. It is the heart defects that make up the majority, and these are only diagnosable in a hospital pediatric unit.
The second problem I know about, since I have designed and carried out several questionnaire epidemiology studies since the pilot one in Carlingford, Ireland in 2000: it is that people can’t remember back even five years, let alone 15 years. And in a situation like Iraq, where having a child with a congenital defect means that you yourself are contaminated and damaged, the likelihood is that you will shortly be dead from cancer and a whole range of illnesses generated by the causes that killed your baby. So the questionnaire study loses cases as you go back in time. The WHO results clearly show this, since the rates they report are actually lower than expected, suggesting that living in Iraq is good for birth outcomes. They seem surprised by this.
So a hospital-based prospective study is the only way. And since this is such a political issue, I said I would only be involved if I could have a hands-on role so that the numbers could be checked, and that was the end of our communication.
The result is very shoddy procedure which would not make it into
peer-review. The WHO says that its work and the report was
peer-reviewed by senior epidemiologists at the London School of
Hygiene and Tropical Medicine, but if this is true these
reviewers should be sent packing. The WHO report fails to refer
to any of the studies, like our follow-up papers on uranium in
Conflict and Health and the IMANA congenital anomaly rates one.
There, for example, we looked at the uranium content along long
strands of hair in mothers of birth-defect children and showed
that the concentrations increased back to the time of the US
attacks.
It is fairly easy to show that the WHO results are ridiculous. There was a previous similar study under Saddam’s regime for the period 1994-1999 which is of interest. This study also was not cited in the WHO report but was discussed in our paper which they must have read. The Iraqi child and maternal mortality survey covered 46,956 births in Iraq from 1994-1999. Results were obtained by questionnaires filled out by the mothers and results were given for all children aged 0-4 who died in 1994-1999. Effects found in this period, if due to environmental agents, would, of course, follow exposures in and following the first Gulf War. Using data presented in the tables in this publication it is easy to show that the results indicated a marked increase in deaths in the first year of life with an infant mortality (0-1) rate of 93 per 1,000 live births. Fifty-six percent of deaths in all the children aged 0-5 occurred in the first month after birth, but since the results were from self-reporting, it was difficult to draw conclusions as to the underlying causes of death except in the case of oncology/hematology. For example, the largest reported proportion of deaths in the neonates were listed as "cough/difficulty breathing" which might result from many different underlying causes. The low rates from congenital malformation reported are hardly credible. However, using data published in the report it appeared that the cancer and leukemia death rates in the entire all-Iraq 0-4 group were about three or four times the levels found in Western populations for this age group. These rates were three times higher in the south where depleted uranium was employed in the major tank battles near the Kuwait border (53 per 100,000 per year) than in the north (18 per 100,000 per year) where there was less fighting and where depleted uranium was not employed to such an extent. Furthermore, cancer and leukemia rates were highest in the 0-1 year group, which is unusual; the main peak in childhood cancer is generally found at age 4.
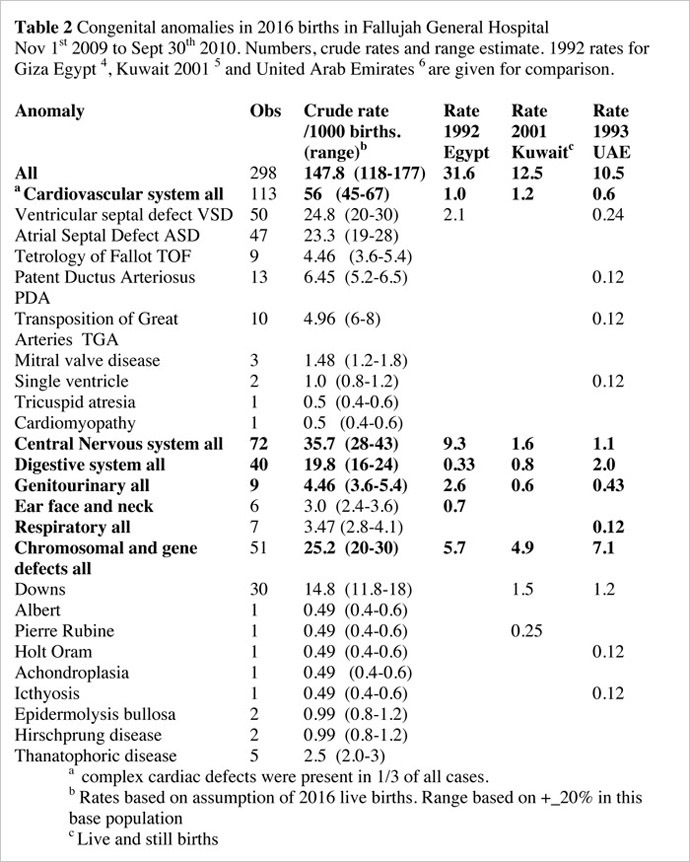
Despite all that can be said about the methodology, it is extremely hard to reconcile the WHO study’s finding of an overall congenital anomaly rate of 23.6 with the rate of 147 we found in Fallujah General Hospital, reported by us in. In Table 2, I copy the full results which were submitted in this congenital anomaly paper. It is clear from this that the majority of conditions could not be recognized by mothers of children who died at or shortly after birth. Of 291 babies with congenital abnormalities in our Fallujah hospital study, 113 were cardiovascular, 40 digestive, 9 genitourinary and 44 chromosomal defects, few of which could be recognized as congenital anomalies by mothers, and would need specialized diagnoses in a top hospital to classify.

It is shown in Table 2 that the rate for congenital heart effects alone is twice the rate reported in the WHO study. Of particular concern is the outcome of the “Expert Peer Group” meeting on 27-28 July, 2013, which apparently endorsed this epidemiologically unsafe approach and its results.
I have written and given presentations on scientific dishonesty. The truth can be established by science, but not if it is dishonest and political. And it seems that this report, and the events and decisions that preceded it, and particularly the London School of Hygiene and Tropical Medicine peer review meeting, are a classical example of scientific dishonesty. The use of the London School of Hygiene and Tropical Medicine reminds me of the use of the Royal Society to produce a disgraceful report on depleted uranium in 2001. Since the outcome is intended to exonerate the US and UK military from what are effectively war crimes, and since the result will be employed to defend the continued use of uranium weapons, all concerned in this chicanery should be put before a criminal court and tried for what they have done. Their actions are responsible for human suffering and death and cannot be forgiven. This is a human rights issue. I returned to the issue of Fallujah when I was invited a second time to make a presentation at the UN Human Rights Council in September 2011. I said then it was time to make a legal stand and I presented the human rights petition I had developed with the International Committee for Nuclear Justice. This issue will be taken forward by the Low Level Radiation Campaign in the next six months, so watch this space.
Finally, we should not forget that the WHO signed an agreement in 1959 with the International Atomic Energy Agency to keep their noses out of any research that has a connection with radiation or radioactivity. This agreement is still in force and is a matter of deep concern.
The statements, views and opinions expressed in this column are solely those of the author and do not necessarily represent those of RT.
The statements, views and opinions expressed in this column are solely those of the author and do not necessarily represent those of RT.